105-year-old sprints the 100m
Posted on April 19th, 2016 by Andries Lodder
Inspirational! The importance of staying healthy and active!
Posted on April 19th, 2016 by Andries Lodder
Inspirational! The importance of staying healthy and active!
Posted on April 18th, 2016 by Andries Lodder

Article by Matt Blake – Charles Eugster is the greatest British sprinter you’ve probably never heard of. He currently holds world records in the 200m (indoor) and 400m (outdoor) sprints, as well as British records in the 60m (indoor), 100m (outdoor), and 200m (outdoor). A couple of weeks ago, he narrowly missed out on the world record for the 60m sprint after pulling his hamstring halfway through. He still won the race to become European Champion. It’s an impressive record, given that the man—by pretty well established standards—shouldn’t be able to cross a road without help, let alone run. He is 96 years old.
The London-born ex-dentist, who now lives in Switzerland, is arguably the fittest senior citizen on the planet. He’s also a body-builder, a public speaker, a writer, a rower, a wakeboarder, an entrepreneur, and a budding fashion designer, planning his own line in elderly couture. But more than anything, he is a professional death defier who hasn’t just slowed the ravages of aging, but reversed them all together: where once white pubic hairs grew, he says, brown ones now flourish.
This was, of course, quite tricky to independently verify when I rang him up recently.
VICE: Hi Charles. Congratulations on the over-nineties 60m European title. Were you disappointed not to get the world record?
Charles Eugster: Oh, very. The thing was, I felt absolutely great before the race and was in my youthful dreams with hopes of attacking the world record of 14.28 seconds. I flew out of the blocks and, after the first 30m, I was out in front of the pack. That’s when my hamstring tore. You see, I was against the most extraordinary people: a 90-year-old German and a 99-year-old Italian. I knew they were quick, but I’d left them miles behind. Then, as the leg pain set in, they started to catch me. I was scared stiff that they would beat me, but of course they didn’t. I staggered over the line within over 18 seconds. Nowhere near the record. Now I must stop training for a month.
Sprinting—or body-building, for that matter—are not things one normally associates with old people. Why?
I was 87 and realized my body was deteriorating. I had a muffin-top waist and my muscles were getting weaker and weaker. I felt so old. But because I was so vain, I didn’t like the idea of it at all. So I joined a body-building gym and employed a personal trainer who was a Mr. Universe to rebuild my body from scratch.
Nine years on, at 96, do you feel old now?
Not at all. I feel like a youngster of 60, tops. Being fit is a wonderful thing. Before I turned 90, I got severe colds every November, but now they’ve completely stopped—I’ve had two in six years. I’ll tell you something else: strength training increases your libido.
And you know this from experience?
Well, you know the story about my pubic hair, don’t you?
I feel like I’m about to.
When I was still training with Mr. Universe, he took me aside one day and asked, “Have you noticed an increase in your libido?” I was embarrassed. I said, “Look, this is not something I’d like to discuss. It’s private.” But he was very persistent, and in the end I relented. I said, “Look now, you mustn’t tell anybody else, but what I’m about to tell you is very dramatic. Incredible. Since I started on this program, my pubic hairs, which were white, have turned brown.” I mean, wow!
So you’ve literally reversed the process of aging.
Yes! You see, the stupid thing is that people don’t realize that you can have a beach body at 90 and turn the heads of the sexy 70-year-old girls on the beach. I am living proof that, if you eat right and exercise properly, you can be that guy at any age.
What do you eat to stay in shape?
Variety is key. I start every day with a protein shake because, as you get older, your protein synthesis no longer functions as well. I avoid sugar and eat lots of meat, especially fat. I’ve been on a fat trip lately. Fat! Piles of fat. Yet, I was in a supermarket the other day and was perplexed to find yogurt with zero fat. What on earth is that? The idea of the nutrition pyramid where, at the top, is a little fat and meat, and at the bottom a lot of carbohydrates, is, excuse me, bullshit. Humans are so unbelievably stupid that we have begun to tinker with food. Our theories of nutrition have resulted in a pandemic of obesity. Can you imagine a hunter-gatherer enjoying a low-fat yogurt? Let me tell you this, too: I read a report recently which said that a fatty diet also increases your libido.
I know you sadly lost your second wife, Elsie, 15 years ago. But with all this talk of libido, are you looking for love?
Yes. But the only problem is that I seem to be so busy with so many other things I don’t have an enormous amount of time. I’m registered with a dating agency, but all they can produce are young things of about 70! Above 70 there’s nothing.
Why is that, do you think?
Because people of 70 to 100 years old are absolutely the lost population. We are ignored by society, by medicine, by research. And we can’t get a job. Nobody cares about us. I’ll give you one silly example: there are no training plans, or gyms, for anybody over 70, as there are in Japan. The way we treat the elderly today is disgraceful. And don’t even get me onto retirement.
What about retirement?
Retirement is the biggest killer of old people, full stop. I prefer to call it involuntary unemployment. What I’m nearly bursting a blood vessel about is the fact that humans are blissfully ignoring the aging process. We recycle everything nowadays, except human beings. Our expiry date is 65, after which we’re thrown on the rubbish heap and chemically treated. We are pouring the experience, creativity, and talent of people over 65 down the toilet. They should be able to found companies, be creative. They have nothing to do except sit about and get sick. This is a world problem and it needs to change.
What’s your answer?
PUT. OLD. PEOPLE. TO. WORK! One of the things I want to do is set up a retraining program for older people. I’d like to see companies set up in old people’s homes that offer, say, computer services. For example, if I want to find out something, the computer is a wonderful thing, but sometimes it takes a while to find [what you’re looking for]. Now, if I could call up an old people’s home and say, “I want this information by that time,” if they have 50 old people working on computers, one of them is bound to come up with something.
Like a sort of elderly IT sweatshop?
[Laughs] Well, we’d pay them properly, obviously. It could be transcriptions, or research, anything.
You’ve seen a world war, a Cold War, the Great Depression, and god knows how many financial crises, not to mention all the good things that have happened since you were born in 1919. What’s the one piece of advice you’d give to young people today?
Explore your talents and never stop learning. In your lifetime you will not have one job, but you will have a huge number of different jobs in different areas. We are at the very beginning of the digital age, of which nobody really knows the consequences. Oh, and don’t get too wrapped up in the culture of youth. Youth is so fantastic, but we should be impressing on people how wonderful, stupendous, exciting, and amazing old age can be, too. Oh, exercise and eat lots of fat. You know why!
What else is on your bucket list?
I want to change the world. I’m writing a book called 97 and Loving It, which I hope to publish this year. Then I want to establish fitness centers for those over 70 and start a job creation company to retrain older people. Then, of course, I want to have some connection with nutrition for the old. And the other thing in the back of my mind is that I would like to create a fashion label for older people. Because the way that older people dress is absolutely disgusting. I don’t just want a label, I want a whole conglomerate.
And what about your sprinting?
Well, once this hamstring heals, I think we’ll see what can be done about the 100m outdoors. There’s a 105-year-old Japanese sprinter called Hidekichi Miyazaki who I would like to run against over 100m. They call him “The Golden Bolt,” and with our combined ages of over 200 years, I think that would be some spectacle!
Original Article by Matt Blake Follow him on Twitter @mattblakeUK
Posted on March 30th, 2016 by Andries Lodder

Jan Withaar during the Gauteng XCO Cup Series #3 at Wolwespruit Track in The City of Tshwane
Posted on March 15th, 2016 by Andries Lodder
HYPERTHYROIDISM
By Dr Kershlin Naidu, Endocrinologist and Specialist Physician, Netcare Waterfall City Hospital
 Last month, we focused on Hypothyroidism where the thyroid gland does not produce enough thyroid hormone. This month’s article discusses an overactive thyroid.
Last month, we focused on Hypothyroidism where the thyroid gland does not produce enough thyroid hormone. This month’s article discusses an overactive thyroid.
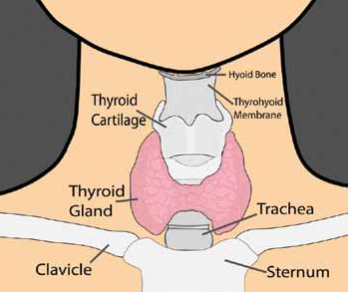
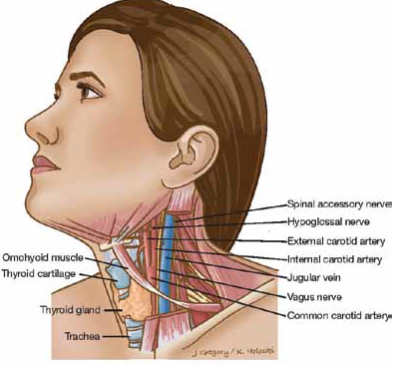
To recap, the thyroid gland is a butterfly-shaped endocrine gland that is normally located in the lower front of the neck. The thyroid makes thyroxine, which is secreted into the blood and then carried to every tissue in the body. Thyroxine is a body chemical (hormone) that is circulated around the body in the bloodstream. It helps to keep the body’s functions (the metabolism) working at the correct pace. Many cells and tissues in the body need thyroxine to keep them functioning correctly. Thyroxine helps the body use energy, stay warm and keep the brain, heart, muscles, and other organs working as they should.
Hyperthyroidism is a condition where the thyroid produces more thyroxine than is needed by the body. It is also referred to as thyrotoxicosis, or an over-active thyroid. It can occur if you have:
It can also occur when too much replacement thyroxine (levothyroxine) is taken as a treatment for an under-active thyroid (hypothyroidism). Hyperthyroidism is more common in women. About 8 in 100 women and 1 in 100 men develop hyperthyroidism at some stage of their lives. It can occur at any age.
SYMPTOMS OF HYPERTHYROIDISM INCLUDE:
Most people with hyperthyroidism do not have all the symptoms but a combination of two or more is common. Symptoms usually develop slowly over several weeks. All the symptoms can be caused by other problems and so the diagnosis may not be obvious at first. Symptoms may be mild to start with but become worse as the level of thyroxine in the blood gradually rises.
CAUSES OF HYPERTHYROIDISM
Graves’ disease
This is the most common cause of hyperthyroidism. It is not clear why Graves’ disease develops in most people, although it is more common in certain families. There may also be family members with other autoimmune diseases (eg. diabetes, rheumatoid arthritis and myasthenia gravis).
Graves’ disease is an autoimmune condition. The immune system normally makes antibodies (tiny proteins that travel in the bloodstream) to attack bacteria, viruses and other germs. In autoimmune diseases, the immune system makes antibodies against tissues of the body. In Graves’ disease the body’s immune system turns against the thyroid gland and produces an antibody that stimulates the thyroid gland to produce too much thyroid hormone. Autoimmune thyroid disease has a strong genetic component. It is thought that something triggers the immune system to make these antibodies. The trigger is not known. Stress also seems to play a role and sometimes people with Graves’ disease may have experienced major stresses in their lives a year or so before Graves’ disease is diagnosed.
Graves’ disease is most common in women between the ages of 20 and 40 years, but can occur at any age in men or women. The thyroid gland enlarges (called a goitre) and makes excessive amounts of thyroid hormone, causing symptoms of hyperthyroidism.
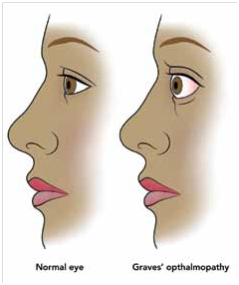
Some people develop eye problems (called Graves’ ophthalmopathy or orbitopathy), which causes dry, irritated or red eyes, and in severe cases may cause double vision. Others develop swelling behind or around the eyes that causes the eyes to bulge out, or inflammation of muscle in the eyelids that can cause excessive lid opening. The more severe manifestations of Graves’ eye disease are uncommon, except in smokers.
 Thyroid Nodules
Thyroid Nodules
This is a less common cause of hyperthyroidism and is characterized by one or more nodules or lumps in the thyroid that may gradually grow and increase their activity so that the total output of thyroid hormone into the blood is greater than normal. This condition is known as toxic nodular or multinodular goitre.
Thyroiditis
Painless (“silent or lymphocytic”) thyroiditis and postpartum thyroiditis are disorders in which the thyroid becomes temporarily inflamed and releases thyroid hormone into the bloodstream, causing hyperthyroidism.
Postpartum thyroiditis can occur several months after delivery. The hyperthyroid symptoms may last for several months, often followed by several months of hypothyroid symptoms, such as fatigue, muscle cramps, bloating, and weight gain.
Subacute (granulomatous) thyroiditis is thought to be caused by a virus. It causes a painful, tender, enlarged thyroid gland. The thyroid becomes inflamed and releases thyroid hormone into the blood stream; the hyperthyroidism resolves when the viral infection improves, and may also be followed by several months of hypothyroid symptoms.
Other causes
Taking too much thyroid hormone medication for hypothyroidism. Some people who take the medicines amiodarone and lithium may develop hyperthyroidism. There are various other rare conditions that result in excess thyroxine being made.
DIAGNOSIS OF HYPERTHYROIDISM
A blood test can diagnose hyperthyroidism. A normal blood test will also rule it out if symptoms suggest that it may be a possible diagnosis. One or both of the following may be measured in a blood sample:
Other tests are sometimes done to clarify the situation and the cause. For example, another blood test that measures T3 is sometimes helpful and an ultrasound scan of the thyroid or a thyroid scan may be done if you have a nodular goitre. In people with Graves’ disease a blood test may detect specific autoantibodies which are commonly raised.
POSSIBLE COMPLICATIONS
If you have untreated hyperthyroidism:
With treatment, the outlook is good. With successful treatment, most of the symptoms and risks of complications go.
TREATMENT OF HYPERTHYROIDISM
The main aim of treatment is to reduce your level of thyroxine to normal. Other problems, such as a large goitre (thyroid swelling) or associated eye problems, may also need treatment. Factors such as the underlying cause of the problem, your age and the size of any goitre are taken into account to decide on the best treatment plan.
Treatment options include the following:
Medicines (carbimazole / neomercazole) Carbimazole reduces the formation of thyroxine by an overactive thyroid gland. It may take 4 to 8 weeks of treatment for your thyroxine level to come down to normal. The dose of carbimazole needed to keep the thyroxine level normal varies from person to person. A high dose is usually given initially which is then reduced as your thyroxine levels come down.
Carbimazole can, rarely, affect your white blood cells which fight infection. If you develop a fever, sore throat, mouth ulcers or other symptoms of infection whilst taking carbimazole, you should stop taking it and see a doctor urgently for a blood test.
RADIOIODINE
This involves taking a drink, or swallowing a capsule, which contains radioactive iodine. The main use of iodine in the body is to make thyroxine. Therefore, the radioactive iodine builds up in the thyroid gland. As the radioactivity is concentrated in the thyroid gland, it destroys some thyroid tissue which reduces the amount of thyroxine that you make. The dose of radioactivity to the rest of the body is very low and is not dangerous. However, it is not suitable if you are pregnant or breast-feeding. In addition, after treatment, women should not become pregnant for at least six months and men are advised not to father children for at least four months.
Your specialist will give detailed advice regarding this form of therapy.
SURGERY
This involves removing part of your thyroid gland. It may be a good option if you have a large thyroid swelling (goitre) which is causing problems in your neck. If too much thyroid tissue is removed then you will be given thyroxine tablets to keep your thyroxine level normal. It is usually a safe operation but, as with all operations, there is a small risk.
TREATMENT FOR EYE PROBLEMS
You may need to see an eye specialist if you develop the eye problems of Graves’ disease. Relatively minor symptoms affect the eyes in about half of people with Graves’ disease. Measures such as artificial tears, sunglasses and eye protectors whilst you sleep may be sufficient to help.
However, about 1 in 20 people with Graves’ disease have severe eye changes. Treatment can then be more difficult and may include surgery, radiation treatment or steroid tablets. If you smoke, it is important that you try to stop. Smoking can actually make your eye problems worse.
BETA-BLOCKERS
Some people are given a beta-blocker medicine (eg. propranolol, atenolol, etc) for a few weeks whilst the level of thyroxine is reduced gradually by one of the above treatments. Betablockers can help to reduce symptoms of tremor, palpitations, sweating, agitation and anxiety.
Regular checks are recommended, even after you finish a successful treatment. It is very important to have regular blood tests to check that you have the right level of thyroid hormone (thyroxine) in your blood. This is because some people become hyperthyroid again at some time in the future. Others who have been treated successfully develop an underactive thyroid in the future. If this occurs, it can usually be treated easily with thyroxine tablets.
TO SUMMARISE
Hyperthyroidism is a condition where the thyroid produces more thyroxine than is needed by the body. Symptoms vary greatly amongst individuals and a diagnosis can be established with a blood test. Hyperthyroidism can be successfully treated with medication, radioactive iodine therapy or surgery.
Dr Kershlin Naidu
B.Med.Sci(NATAL), MBBCh(WITS), FCP(SA), MMed(WITS), FSEM(SA)
Endocrinologist / Specialist Physician Netcare Waterfall City Hospital
Room SF218, 2nd Floor, South Block.
Tel: 011 304 6865 (emergency on 011 304 6600
Email: drknaidu@waterfallhealth.co.za
Posted on February 29th, 2016 by Andries Lodder
Do you think you are too old to do exercise? Watch Alan here, he’s 81 years old, and he doesn’t think so! Well done Alan, keep it up!
Posted on February 25th, 2016 by Andries Lodder
HYPOTHYROIDISM
By Dr Kershlin Naidu, Endocrinologist and Specialist Physician, Netcare Waterfall City Hospital

Hypothyroidism is a condition in which the thyroid gland does not produce enough thyroid hormone. It is the most common thyroid disorder.
The thyroid is a butterfly-shaped gland in the middle of the neck, located below the larynx (voice box) and above the clavicles (collarbones). The thyroid produces two hormones, triiodothyronine (T3) and thyroxine (T4), which regulates how the body uses and stores energy (also known as the body’s metabolism). Thyroid function is controlled by a gland in the brain, known as the pituitary. The pituitary produces the thyroid-stimulating hormone (TSH), which stimulates the thyroid to produce T3 and T4.
CAUSES OF HYPOTHYROIDISM
In about 95% of cases, hypothyroidism is due to a problem in the thyroid gland itself and is called primary hypothyroidism. However, certain medications and diseases can also decrease thyroid function. In some cases, hypothyroidism is a result of decreased production of the thyroidstimulating hormone (TSH) by the pituitary gland (called secondary hypothyroidism).
Hypothyroidism commonly develops in adult women and becomes more common with increasing age. Thyroid problems generally occur more commonly in Caucasian than in Black populations. However, it can occur at any age and can affect anyone.
The most common cause of primary hypothyroidism is due to an autoimmune disease called autoimmune thyroiditis (Hashimoto’s thyroiditis). The immune system normally makes antibodies to attack bacteria, viruses, and other germs. If you have an autoimmune disease, the immune system makes antibodies against certain tissues of your body.
With autoimmune thyroiditis, you make antibodies that attach to your own thyroid gland, which affect the gland’s function. The thyroid gland is then not able to make enough thyroxine and hypothyroidism gradually develops. It is thought that something triggers the immune system to make antibodies against the thyroid but the trigger is not known. Some people with autoimmune thyroiditis also develop a swollen thyroid gland (goitre).
Autoimmune thyroiditis is more common in patients with:
Other causes of hypothyroidism include:
SYMPTOMS OF HYPOTHYROIDISM
The symptoms of hypothyroidism vary widely – some people have no symptoms, while others have dramatic symptoms. These symptoms are notorious for being nonspecific and for mimicking many of the normal changes of aging. Usually, symptoms are milder when hypothyroidism develops gradually.
General symptoms – The thyroid hormone normally stimulates the metabolism and most of the symptoms of hypothyroidism reflect slowing of metabolic processes. General symptoms may include fatigue, sluggishness, weight gain and intolerance of cold temperatures.
Skin – Hypothyroidism can decrease sweating. The skin may become dry and thick. The hair may become coarse or thin, eyebrows may disappear and nails may become brittle.
Eyes – Hypothyroidism can lead to mild swelling around the eyes. People who develop hypothyroidism after treatment for Graves’ disease may retain some of the eye symptoms of Graves’ disease, including protrusion of the eyes, the appearance of staring and impaired movement of the eyes.
Cardiovascular system – Hypothyroidism slows the heart rate and weakens the heart’s contractions, decreasing its overall function. Related symptoms may include fatigue and shortness of breath with exercise. These symptoms may be more severe in people who also have heart disease. In addition, hypothyroidism can cause mild high blood pressure and can raise blood levels of cholesterol.
Respiratory system – Hypothyroidism weakens the respiratory muscles and decreases lung function. Symptoms can include fatigue, shortness of breath with exercise and decreased ability to exercise. Hypothyroidism can also lead to swelling of the tongue, hoarse voice and sleep apnea. Sleep apnea is a condition in which there is intermittent blockage of the airway while sleeping, causing irregular sleep patterns and daytime sleepiness.
Gastrointestinal system – Hypothyroidism slows the actions of the digestive tract, causing constipation. Rarely, the digestive tract may stop moving entirely.
Reproductive system – Women with hypothyroidism often have menstrual cycle irregularities, ranging from absent or infrequent periods to very frequent and heavy periods. The menstrual irregularities can make it difficult to become pregnant; and pregnant women with hypothyroidism have an increased risk for miscarriage during early pregnancy. Treatment of hypothyroidism can decrease these risks.
Myxoedema coma – In people with severe hypothyroidism, trauma, infection, exposure to the cold and certain medications can rarely trigger a life-threatening condition called myxoedema coma, which causes a loss of consciousness and hypothermia (low body temperature).
DIAGNOSIS OF HYPOTHYROIDISM
Blood tests can confirm the diagnosis and pinpoint the underlying cause of the thyroid hormone deficiency. The most common blood test for hypothyroidism is TSH (thyroid stimulating hormone). TSH is the most sensitive test because it can be elevated even with small decreases in thyroid function. Thyroxine (T4), the main product of the thyroid gland, may also be measured to confirm and assess the degree of hypothyroidism.
TREATMENT OF HYPOTHYROIDISM
The goal of treatment for hypothyroidism is to return blood levels of TSH and T4 to the normal range and to alleviate symptoms. The treatment for hypothyroidism is thyroid hormone replacement therapy. This is usually given as an oral form of T4. Generic (levothyroxine) and brand-name (Euthyrox®, Eltroxin®, Synthroid®) formulations are equally effective. However, it is preferable to stay on the same type of T4 rather than switching between brand name and/or generic formulations. If a switch is necessary, a blood test is usually done six weeks later to determine if the dose needs to be adjusted.
Some clinicians prescribe another form of thyroid hormone, triiodothyronine (T3) in combination with T4. Selected patients may benefit from T3 therapy. Depending on the severity of the hypothyroidism, improvement in symptoms may be seen within a few weeks to months after the initiation of therapy.
If you have untreated hypothyroidism:
SURGERY
Hypothyroidism can increase the risk of certain surgery-related complications; bowel function may be slow to recover and infection may be overlooked if there is no fever. If preoperative blood tests reveal low thyroid hormone levels, non-emergency surgery is usually postponed until treatment has returned T4 levels to normal.
HYPOTHYROIDISM WITHOUT SYMPTOMS
In some cases, hypothyroidism is extremely mild or causes no obvious symptoms (called subclinical hypothyroidism). The decision to treat subclinical hypothyroidism with T4 is controversial and is dependent on many patient factors. Your doctor will be able to advise you on treatment options.
IN CONCLUSION
Hypothyroidism is a common disorder. Symptoms develop gradually and may be confused with other conditions. The diagnosis of hypothyroidism can be easily made with a blood test. Treatment with levothyroxine is easy, cheap and effective.
Dr Kershlin Naidu
B.Med.Sci(NATAL), MBBCh(WITS), FCP(SA), MMed(WITS), FSEM(SA)
Endocrinologist / Specialist Physician Netcare Waterfall City Hospital
Room SF218, 2nd Floor, South Block.
Tel: 011 304 6865 (emergency on 011 304 6600
Email: drknaidu@waterfallhealth.co.za
Posted on February 16th, 2016 by Andries Lodder
Original Article by Brigitte Mileson
An inside view to athletes…. Almost like a food critic.. All opinions are my own.
Who is Jean Spies…….
This sounds terrible, but I have been struggling to remember when I first met him. I knew and worked on his father first and then he became one of my clients as well. When I say worked on, I mean sports massage, because that’s what I do.
I recall helping with his shoulder injury as massaging and flushing the area is a great promoter of healing but it wasn’t until about one year ago I actually got to know him. Some people say he is an incredible guy, others say they don’t really know much about him, others say they find him a little brash and loud, but some love his sense of humour. What I am going to tell you is that, in my opinion all of it is true.
Jean first came across to me a little abrupt, maybe slightly arrogant, but a seemingly happy, genuine guy. As we spent a bit more time in each other’s company either during the regular weekly massage session or at the races, I began to see a different side to him. A side not many people would see unless they took the time to see it. Jean is an incredibly private person. He likes to keep all the aspects of his life separate. Not many people know how much he actually does and what he is involved in, so here is a short and sweet description. Other than riding all bicycles, road and track and mountain bike, Jean is in fact a very religious man, and has several different yet close groups of friends with whom he shares his time.
He works part time at Design in Motion bicycle store building bikes and doing setups, he instructs classes at Watt Lab twice a week, he helps his father with his business and if that isn’t enough he fits in two to three training sessions pretty much every day.
When I asked him why he keeps things separate? His answer to me was “to keep life simple.” Sounded strange to me initially, but if you think about it each different area of your life makes you who you are, if you identify what makes you happy you become a whole person. Those different areas don’t necessarily have to overlap to have more or less meaning. Interesting theory, I am sure one that can spark some debate.
Recently Jean gave up personal time to help out at a track development training Camp in Durban, he doesn’t receive monetary compensation for this, however his excitement and softer side showing with simple things like teaching the youngsters how to ride rollers was clearly visible.
Jean does likes things done a certain way, hell, he apparently even likes his coffee made in a certain manner. He proudly says he is ADHD and OCD. Meaning he likes things perfect but only until he is distracted with something else. That’s why he is such a great track cyclist. ‘Maximum perfection in a short amount of time.’ This proven by having twelve National titles and multiple podiums, including ones overseas by the age of 26.
When I asked him about his successes, although proud of them his reply was, “You are only as good as your last race.” A comment I have become accustomed to in the cycling world.
Jean has gone through a relatively trying three years. A crash saw his shoulder dislocated, but it shouldn’t have been that bad right? Wrong, eventually after multiple dislocations he eventually underwent surgery. As any athlete knows, any injury plays havoc on your mental state and your trust of your body to perform. He battled during this time, with the desire to ride but the unknown of how his shoulder would hold up. Eventually racing competitively at SA Champs last year renewed his desire to race, but not only race, to race hard and taste victory again.
Victory came but not where he expected. He competed in the Omnium Champs towards the end of last year. This is an event where you have to consistently do well in all six events to win. It is pretty tactical because there is a whole lot of points involved. Jean has always classified himself more as an endurance rider not a sprinter, so winning the Kilo – a sprinters race, came as a bit of a surprise. He also did incredibly well in the flying lap, 2nd by splits. These two events are short and fast. The Kilo is literally ride as hard as you can for one kilometre and the fastest man wins. The Flying lap is same principle just shorter. 250m only.
This surprising result was possibly the best thing for him, as he saw it as new challenge and it gave him the desire to compete and get to the highest level of racing in the world again. A desire that had been wavering due to not only injury but also politics.
Jean has in the last three weeks, has gone about privately funding a trip to African Continental Championships in Morocco, as Cycling South Africa does not have budget to send a team. Why go through all the fuss of getting to Morocco for African Championships? As African Continental Champion you gain automatic entrance into World Championships and as Jean explains with excitement, he would get to race on one of the best wooden tracks in the world, against the best in the World, what could be better than that?!
What are the chances of Jean succeeding at African Continental Champs? In my personal opinion, being privy to the amount of preparation he has done and dedication he has shown, I say he stands as good a chance as anyone, if not more because he has talent and experience to call upon.
Like him, don’t like him, but as an athlete he has proven to be one of the best in the recent past and who knows what the future holds for him.
He has an athlete page on FaceBook which he is updating daily about his journey and racing especially at the moment in Morocco. This will hopefully continue with an adventure of racing at World Champs. Feel Free to check it out. – Jean Spies Track Cyclist.
Best of Luck Jean!


Posted on February 9th, 2016 by Andries Lodder
Rheumatoid Arthritis is one of many types of arthritis, and is a degenerative disease that typically impacts the joints of the knees, hips, feet, spine and hands.
Rheumatoid Arthritis is inflammation in the lining tissue of the joint, called lymphocytes. This in turn causes swelling and damage to both the cartilage and bone.
Rheumatoid Arthritis is the most common form of inflammatory arthritis and even though anyone can get it, it is most commonly found in women above the age of 40.
Some common symptoms of Rheumatoid Arthritis are:
Many people with Rheumatoid Arthritis can control their pain and the disease with medication and exercise. Exercise reduces joint inflammation and pain, maximizing joint function and preventing joint destruction and deformity.
Regular controlled low impact exercise is important to maintain joint mobility and strengthening of the muscles around the joints. Swimming is form of exercise that is particularly helpful because it allows exercise with minimal stress on the joints.
For an individualized exercise program to help you control your symptoms, give us a call.
Posted on January 27th, 2016 by Andries Lodder
Diabetes is a metabolic disease which is marked by high levels of sugar in the blood. It is either caused by the body producing too little insulin, the cells being resistant to insulin or by both.
Exercise helps in the control of blood glucose levels, because in the absence of insulin, exercise will enhance the uptake of glucose.
Most of the foods that we eat are broken down into glucose, which passes into the bloodstream and is used by the cells for growth and energy. The glucose in the bloodstream is known as blood sugar. The body attempts to keep this blood sugar level constant for normal body function.
When a person has diabetes one of two things can happen to prevent glucose storage, the pancreas either secretes to little or no insulin or the cells do not respond to the insulin secreted. This causes glucose to build up in the bloodstream and eventually is passed out of the body in the urine. This build up of glucose in the blood leads to damage of the small blood vessels.
Some people may even have pre-diabetes. These people have blood glucose levels higher than normal but it is not high enough for them to be diagnosed as diabetics.
Fasting Blood Glucose (mmol/L) | Classification |
3.9 – 5.5 | Normal Glucose Tolerance |
5.6 – 6.9 | Pre-Diabetes |
>7.0 | Diabetes |
Type 1 Diabetes
Type 2 Diabetes
Diabetes cannot be cured. The short-term goals for treatment are the stabilization of high blood sugar levels. The long-term treatment goals include the relieving of symptoms, prevention of diabetes-related complications and to prolong life.
People with diabetes should not only keep their blood glucose levels under control, but also their blood pressure and cholesterol levels.
Benefits of exercise:
Exercise prescriptions are individualized to meet the person’s medication schedule and severity of any diabetic complication and also to the goals and expected benefits that the exercise program may hold. Always drink adequate amounts of fluids during exercise and always keep a source of rapidly acting carbohydrates available.
If you have any questions about Diabetes, don’t hesitate to contact me.
Posted on January 11th, 2016 by Andries Lodder
![]()
We have a new face here at The Gym, and her name is Debra.
Debra is a Registered Physiotherapist who has recently relocated to Gauteng from Howick in the KZN Midlands.
She worked as a physio in private practice in Howick and has also been the physiotherapist at Michaelhouse School for the last 17 years.
Debra has a strong interest in sports physiotherapy but also treats people of all ages with physical problems caused by illness, accident or ageing.
Debra herself is a keen runner and triathlete and has completed 5 Comrades Marathons and numerous triathlons, including a full Ironman.
Debra utilizes skilled hands on physiotherapy including neural tissue mobilisation, myofascial and connective tissue release, triggerpoint therapy and spinal joint mobilisation and manipulation. This hands on therapy is augmented by other modalities such as dry needling, neuropropriceptive taping and electrotherapy (eg, ultrasound / interferential)
For more details on Debra’s practice, please don’t hesitate to contact her. All her details can be found on her webpage. Just click on the link: Debra Ludgater Physiotherapy
Welcome to the family and may your practice just prosper here with us!